{{title}}
{{description}}
As a patient of Citizen Potawatomi Nation Health Services, you have the right to:
- Timely access to medical and health-related services which meet standards of care, and which are delivered with respect and recognition of your cultural and spiritual values
- A patient/practitioner relationship conducted in an environment where your privacy and the confidentiality of your relationship are guarded by every employee.
- A clear explanation of your condition, diagnoses, treatment plan, therapy options, and prognosis
- Participate in decisions about your care and receive clear answers to your questions.
- Refuse treatment and to receive an explanation of the consequences of your refusal.
- An explanation of charges levied for your care, and how reimbursement issues will be resolved.
- Make comments or complaints concerning your care and to have your inputs acted upon.
- Know the professional standing and licensure status of individuals providing your care.
- Decide for yourself whether or not you will participate in clinical trials or investigative studies without fear of retribution of any kind.
- An explanation of Advance Directives for Healthcare (Living Wills), appointing someone you trust to help you make decisions on your care.
In addition to the rights listed above, it is your responsibility to:
- Give your practitioners complete and accurate information about your personal and family medical history, present health status, and other information needed to make prompt, accurate diagnoses.
- Notify your practitioner if you don’t understand your condition, treatment plan, instructions for taking medications, or other information given to you by your care givers and counselors.
- Follow instructions, treatment plans, and therapy regimens given to you by CPNHS practitioners.
- Inform clinic staff when you obtain or lose health benefit coverage.
- Pay billed charges in a timely manner, health insurance and tribal benefit will be applied (if applicable).
- Keep appointments or notify the clinic at least 24 hours prior if you must cancel an appointment.
- Conduct your visit in a manner which fosters good order and consideration of others.
- Adhere to the established COVID-19 policies of CPN Health Services.
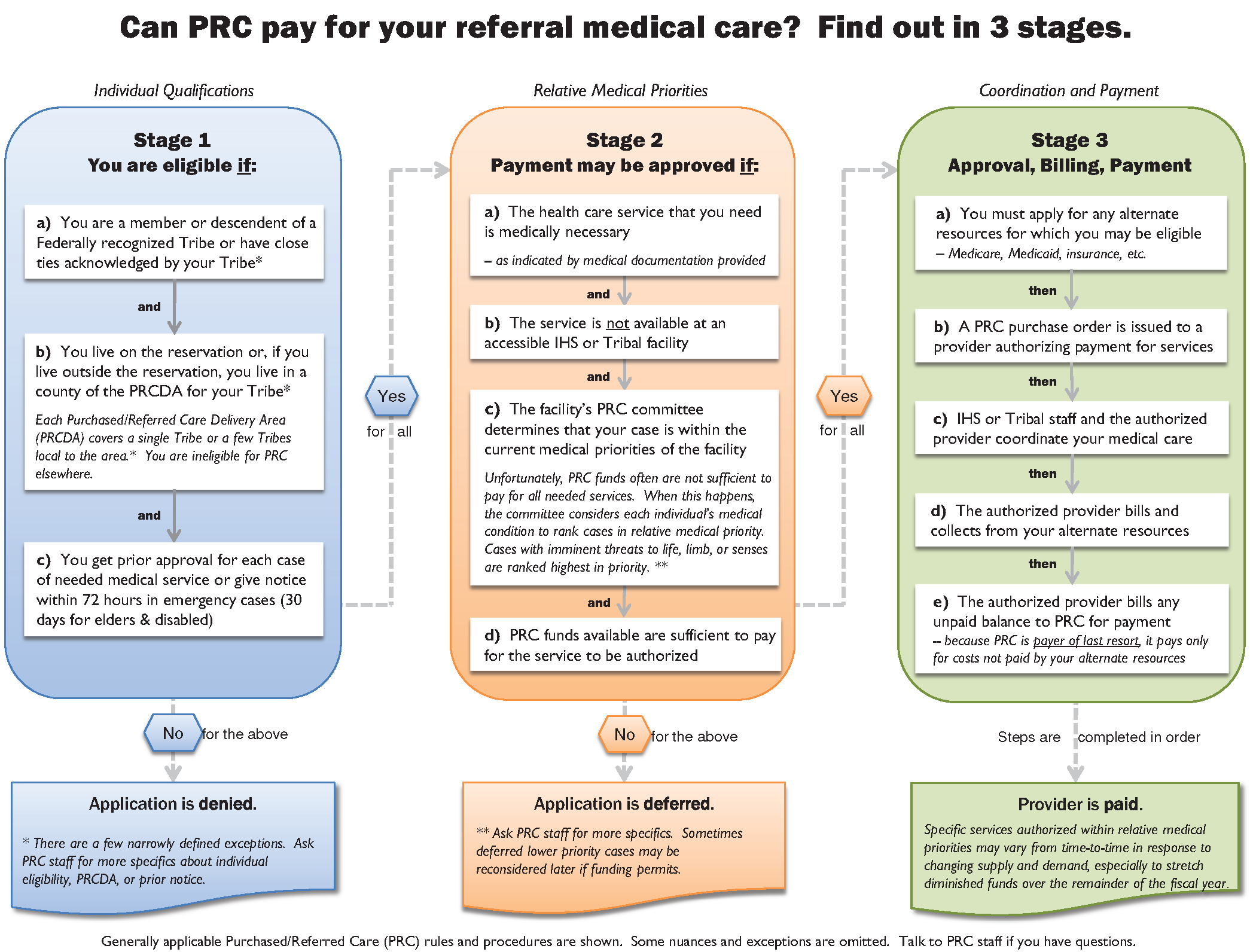
What is Purchased/Referred Care?
Purchased/Referred Care (PRC) exists to supplement or complement other health care resources available to Native Americans. PRC funds are used when no direct care exists or is not capable of providing required emergency and/or specialty care.
PRC is required to operate within appropriated funds. There is no requirement to provide payment for services under the PRC program unless funds are available.
PRC is not:
- An Entitlement Program
- An Insurance Program
Does CPN PRC have unlimited funds?
No. PRC resources are based on a limited congressional appropriation (or budget).
When are PRC funds used?
PRC funds are used in situations where:
- No IHS direct care facility exists.
- The direct care facility cannot provide the required specialty care.
- The direct care facility has an overflow of medical care workload.
PRC is limited to services that are medically indicated within the established medical priorities.
If services are not authorized for payment, they will be denied or deferred.
Previously known as Contract Health, PRC is available in the event services are required beyond what is offered at CPNHS, your primary provider may refer you for services outside of the clinic. With an approved referral and current proof of residency- Purchased/Referred Care (PRC) funds may cover the cost for these medical services and some additional services. The expenditure of PRC services is based on medical necessity and current funding level. Each patient will be assigned to a PRC patient referral clerk based on their last name and insurance. Patients are responsible for notifying referral clerks of all outside appointments prior to the appointment date. Failure to notify may result in denial of payment. Authorized office visit referrals are generally limited to 3 appointments per referral. If continued care is needed beyond the limit set forth a new referral will need to be obtained. If a procedure, surgical or non has been requested by your provider, a separate referral will need to be placed for review. All nonemergent procedures and surgeries require an approved referral prior to scheduling.
PRC eligibility requirements are listed below:
CPN tribal members- Enrolled CPN tribal members who can provide proof of residency within the designated catchment area will be eligible to receive services through PRC.
CPN tribal members must reside within the PRC catchment area of Pottawatomie, Cleveland, Oklahoma, Logan, and Lincoln Counties.
Native Non-CPN member (member of other federally recognized tribe)- must live within the CPN PRC catchment area- south of the North Canadian River, north of the Canadian River, East of Indian Meridian Road, and west of the Pottawatomie County/Seminole County line.
***Patients who do not live in the CPN service area will have all referrals forwarded to their service area to be reviewed and processed.
For all CPN PRC patients, evidence must exist that an alternate resource, such as Medicaid, has been applied for. Such evidence is mandatory and will be obtained once per year due to Federal regulations that require PRC funding only to be used after all other alternative resources have paid. Each patient without a secondary payer will need to apply for Medicaid through a Benefits Specialist- located at your clinic.
If you have private insurance, please notify PRC at least 48-hours prior to your appointment date for a Coordination of Benefits to be sent to the provider.
In the case of emergency room visits, PRC will need to be notified within 72 hours to determine eligibility for payment and must be deemed medically necessary. Medical priorities have been established for determining which referrals can be authorized for payment. Notification does not assure authorization of payment. However, if you do not notify PRC within 72 hours, your bill(s) will not be paid.
Please note that IHS facility emergency room visits are of no cost to patients. Locations include CNMC in Ada, Creek Nation in Okemah, Clinton, Lawton, and Claremore.
**If you receive a bill from a provider, please provide a copy to PRC as soon as possible. You may bring bills to the CPN PRC office located on the 3rd floor of the old Mission Hill Hospital. Please enter on the North side.
CPN PURCHASED/REFERRED CARE
1900 S. GORDON COOPER DR.
SHAWNEE, OK 74801
P: (405) 964-4123
Are There Minor Dependent Children In The Home (Under 19)?
Have Any Household Members Applied For Disability?
Do you have insurance?
Is Pregnant?
Any Catastrophic Illnesses, Such As TB or AIDS?
Do you have internet access?
Are you a migrant worker?
Are you currently homeless?
Are you an employee of CPN?
Are you a member/citizen of a federally recognized tribe?
Do you have a Tribal ID or Certification of Indian Blood Card (CBID)?
Emergency Contact
Next Of Kin
Are you currently or have you in the past served in the United States military?
Are you current active duty?
Preferred Clinic Location
* Must select one location before continuing
East Clinic
West Clinic
Clinical Services Requested
Medical
Dental *
Optometry
Behavorial Health *
* Please note that these services require an additional application. Our team is happy to provide these forms to you upon request.
Do you have medical insurance (including Medicare, Medicaid, or Private Insurance)?
Do you have Medicare?
Do you have Medicaid?
Do you have Private Insurance?
Do you have Vision Benefits?
Do you have Dental Benefits?
Note: In Part II, provide information on the policy holder of the patient’s health insurance policy
| Patient's Name | Relationship to Policyholder | Date of Birth | Chart# (if known) | Effective Date |
|---|---|---|---|---|
Allergy to Anesthesia
Anemia/Blood Disorder
Arthritis - Type:
Bed-Wetting After Age 5
Blood Vessel Disorder
Blood Transfusions
Breathing Problem - Bronchitis, Pneumonia
Cancer - Type:
Chickenpox
Constipation Requiring a Doctor Visit
COPD/Asthma
Depression
Diabetes
Drug/Alcohol UseAddiction
Ear, Nose, Throat Problems
Eye/Vision ProblemsBlurred Vision
Frequent Abdominal Pain
Frequent Ear Infections
Gastro-intestinal Reflux
Has Started Menstrual Peroids
Heart DiseaseHeart Murmur
Heart Failure
High Blood Pressure
HIV/AIDS
Incontinenance/Urinary Problems
Kidney Disease/StonesKidney/Bladder Infection
Liver problems/Hepatitis
Nasal Allergies
Neurological Problems or Convulsions
Osteoporosis
Problems with Peroids
Prostate Problems
Seziures/Frequent Headaches
Skin Problems (Acne, Eczema, etc.)
Sleep Apnea/CPAP
Stomach Ulcers/Bloody Stools
Stroke/Blood Clots
Thyroid or Endocrine Disease
Tuberculosis
Other:
Please indicate all previous surgeries you have had (Colonoscopy, EGD, Tubal, Vasectomy, Joint Replacement, Hysterectomy, etc) or hospitalizations
| Year | Procedure/Reason | Surgeon | Location |
|---|---|---|---|
If patient is less than 18 years old: Are Immunizations up to date?
Have you ever injected drugs into your veins?
Do you use any illegal drugs?
Do you have a living will indicating your advanced directive for health care?
Do you want information about a living will?
Please list all prescriptions including any over-the-counter medications. Also list any herbal medications/supplements.
| Name | Dose | Frequency |
|---|---|---|
Alcohol Abuse - Notes:
Anemia - Notes:
Arthritis - Notes:
Asthma - Notes:
Autoimmune Disease (Lupus, RA, etc.) - Notes:
Bed-Wetting After Age 10 - Notes:
Bleeding Problems - Notes:
Deafness - Notes:
Cancer - Notes:
Diabetes - Notes:
Drug Abuse - Notes:
Epilepsy or Convulsions - Notes:
Heart Disease - Notes:
High Blood Pressure - Notes:
High Cholesterol - Notes:
HIV/AIDS - Notes:
Kidney Disease - Notes:
Liver Disease - Notes:
Mental Illness/Depression - Notes:
Mental Retardation - Notes:
Nasal Allergies - Notes:
Neurological Problems - Notes:
Osteporosis - Notes:
Seizures - Notes:
Stroke - Notes:
Thyroid Disease - Notes:
Tuberculosis - Notes:
Additional Family History - Notes:
HOUSEHOLD: Please list all those living in the child’s home below.
| Name | Age | Relationship | Health Problems |
|---|---|---|---|
List siblings not listed above and state their age and where they live:
If parents are separated or not living with the child, what is the child’s custody status?
If a parent lives outside the home, how often does the child see that parent?
BIRTH HISTORY
Did Mother Smoke While Pregnant?
Use Alcohol?
Use Drugs?
GENERAL HEALTH HISTORY
DEVELOPMENT
SCHOOL
Effective August 10, 2011
The Privacy Rule of the Health Insurance Portability and Accountability Act (HIPAA) of 1996 require that you, our patient, be informed about how your protected health information (PHI) is used and disclosed by the CPNHS, and how you can get access to your individually identifiable health information (IIHI). PLEASE READ THIS NOTICE CAREFULLY!
THE CPNHS/CPN WEST COMMITMENT TO PROTECTING YOUR PRIVACY
CPNHS employees protect the privacy of your IIHI. In the normal course of providing your care we create records regarding you and the nature of your visits. We are required by law and bound by professional ethics to keep information about you confidential and private. This statement describes our obligations to you and the privacy practices we employ to protect your IIHI. We are ethically and legally bound to observe the terms of this notice or of subsequent Privacy Practices Notices which might replace it. We reserve the right to change this Privacy Practices Notice and any revision or amendment will be applicable to all records we create or maintain concerning you in the future. A copy of the current Notice will be posted in the reception area and you are welcome to a copy of your own. If you have questions about this Notice, please contact the Privacy Officer by mail at 2307 S. Gordon Cooper Dr., Shawnee, OK 74801.
CPNHS/CPN WEST USES AND DISCLOSURES OF YOUR IIHI
TREATMENT. Information gained from examinations and diagnostic tests will be used to diagnose and treat you. For example, we may ask you to have an X-ray made, and we may use the results to diagnose your injury or illness. We may disclose this information to others who are involved in your care and treatment including family members.
PAYMENT. We may use and disclose information about you in order to bill and collect payments from public and private healthcare insurers and payers for services rendered to you. For example, if you have health insurance, we may exchange information about your visits with your insurer in order to obtain reimbursement from them.
HEALTHCARE OPERATIONS. We may use and disclose data concerning you during the routine performance of functions related to our practice of medicine, dentistry, and public health activities. These functions include the peer review and quality assurance programs, practice management activities, financial management actions, and case management processes. For example, we may use information about you to call and remind you of an appointment, and we may discuss your IIHI to establish treatment plans and therapy options.
Under a limited number of specific circumstances, we may use or disclose your protected health information without your consent. These circumstances include:
PUBLIC HEALTH RISKS. The CPNHS may disclose your IIHI to public health authorities allowed by law to have the information for (a) maintaining vital records; (b) reporting cases of abuse, neglect, and abandonment; (c) preventing or controlling disease, injury, or disability; (d) notifying individuals of potential exposure to a communicable disease; (e) reporting adverse reactions to drugs or medical devices; (f) communicating with your employer concerning workplace-related illness or medical surveillance.
HEALTH OVERSIGHT ACTIVITIES. The CPNHS may disclose your IIHI to a health oversight agency with a legal right to have it. Oversight activities include (a) investigations; (b) inspections; (c) audits; (d) licensure and disciplinary actions; (e) civil, administrative, and criminal proceedings; and (f) activities necessary for monitoring government-sponsored programs, and (g) compliance with civil rights laws.
LAWSUITS AND SIMILAR PROCEEDINGS. The CPNHS may use and disclose your IIHI in response to court or administrative orders and subpoenas. We will always try to notify you of the request so that you can take whatever actions you deem appropriate. We may disclose your IIHI if asked to do so by a law enforcement official in connection with (a) a crime victim; (b) a death resulting from criminal conduct; (c) criminal conduct occurring at the CPNHS/CPN West facility; (d) identifying or locating a suspect, material witness, fugitive, or missing person; or (e) in an emergency to report a crime.
THREATS TO HEALTH OR SAFETY. The CPNHS may disclose or use your IIHI to reduce or prevent threats to your health or safety or the health and safety of another person or the general public.
MILITARY OR NATIONAL SECURITY. The CPNHS may disclose your IIHI if you are a member of the U.S. or foreign military forces if asked to do so by the appropriate authorities. We may also divulge your IIHI to federal officials for reasons related to the security of the nation, the protection of the President or other officials or foreign heads of state.
INCARCERATION. The CPNHS may disclose your IIHI to corrections officials if you are incarcerated (a) to assist the institution to provide health services to you; (b) for the safety of the institution; and to (c) protect the health and safety of other individuals in the institution.
WORKERS’ COMPENSATION. The CPNHS may disclose IIHI to workers’ compensation officials.
YOUR RIGHTS REGARDING YOUR IIHI
You have the following rights regarding the IIHI the CPNHS produces or maintains about you:
CONFIDENTIAL COMMUNICATION. You may request the CPNHS communicate with you in a particular manner or a specific location. For example, you may ask that we contact you at work rather than at home. You needn’t give a reason for your request, and we will give you a CPNHS Form 700-9b for expressing your wishes. We will honor reasonable requests but you may have to pay if there are costs associated with your request.
RESTRICTIONS. You may request the CPNHS restrict the use or disclosure of your IIHI for treatment, payment, or other operations. For example, you can request that your IIHI not be released to certain individuals. Your request must be in writing and you can use the CPNHS Form 700-9b or a letter for your request. We do not have to agree with your request, but if we do agree, we will abide by our agreement.
RECORD COPIES AND INSPECTION. You have the right to view and obtain copies of your IIHI except for psychotherapy notes. Your request must be written and we ask that you use the CPNHS Form 700-4 to request a review of your records and the Form 700-3 to request copies. If we deny you access, you can ask for a review of the denial by a licensed healthcare professional of our choosing.
AMEND RECORDS. You may ask the CPNHS to amend your IIHI if you believe it is incorrect or incomplete. You must request the amendment in writing and we ask that you use the CPNHS Form 700-5 for this purpose. We may deny your request to amend your record if (a) the record is accurate and complete; (b) we don’t have the records you want amended; (c) the record you want amended is not available for your review (i.e. psychotherapy notes); or (d) the record was not created by the CPNHS (unless the author is no longer available to amend the record).
DISCLOSURE EXPLANATION. You have the right to an accounting of certain non-routine disclosures the CPNHS has made of your IIHI for purposes other than treatment, payment, or other related operations. We are not required to document uses of your IIHI for routine patient care purposes. You must submit your request in writing and specify a time period not longer than six (6) years from the date of the disclosure and not earlier that April 14, 2003. One accounting is provided at no cost but we may charge you for additional requests during any 12-month period. We will inform you of the cost before we comply with your request and you may authorize us to continue or you may withdraw the request.
PERSONAL NOTICE. You have the right to a personal copy of this Notice. Ask the receptionist in the central reception area for a copy and it will be provided at no cost.
COMPLAINT. If you believe your privacy rights have been violated, you may complain to the Director, CPNHS or to the Secretary of the Department of Health and Human Services. Complaints to the CPNHS must be submitted in writing to the Privacy Officer, 2307 S. Gordon Cooper Drive, Shawnee, OK 74801. You will not be penalized for filing a complaint.
AUTHORIZATION. The CPNHS will obtain your written authorization for uses and disclosures of your IIHI which are not addressed by this Notice or permitted by law. You can revoke any authorization you give us at any time by submitting the revocation in writing to the CPNHS Privacy Officer.
On behalf of the providers and staff of Citizen Potawatomi Nation Health Services, we welcome you to our practice. We are honored that you have entrusted us with your care. Included in this \ packet you will find a new patient form, information on Purchased Referred Care (formally Contract Health), as well as disclosure and confidentiality forms.
The documents listed below should be submitted with your new patient paperwork. As a tribally operated facility, these documents allow us to determine if the patient meets eligibility requirementsfor care within our clinics. Failure to include or provide the requested documents will result in delays in access to services within our facilities.
Native American Adults:
- CDIB or Tribal Enrollment Card
- Social Security Card
- Driver's License or State ID
- Health Insurance Card (Front and Back)
CPN Spouses (Non-Native Spouse of a CPN Tribal Member):
- Spouse's CPN Tribal Enrollment Card
- Social Security Card
- Driver's License or State ID
- Health Insurance Card (Front and Back)
- Marriage License
CPN Employees and Their Adult Dependents:
- Employee ID
- Social Security Card
- Driver's License or State ID
- Health Insurance Card (Front and Back)
If you need assistance completing new patient forms or have questions, please call or visit one of the Citizen Potawatomi Nation Health Services clinics listed below. Completed forms and documents may be returned to either clinic facility.
| Patient's Name | Relationship to Policyholder | Date of Birth | Chart# (if known) | Effective Date |
|---|---|---|---|---|
{{item.Name}} |
{{item.Relationship}} |
{{item.DateBirth}} |
{{item.Chart}} |
{{item.EffectiveDate}} |
| Year | Procedure | Surgeon | Location |
|---|---|---|---|
{{item.Year}} |
{{item.Procedure}} |
{{item.Surgeon}} |
{{item.Location}} |
| Name | Dose | Frequency |
|---|---|---|
{{item.Name}} |
{{item.Dose}} |
{{item.Frequency}} |
